
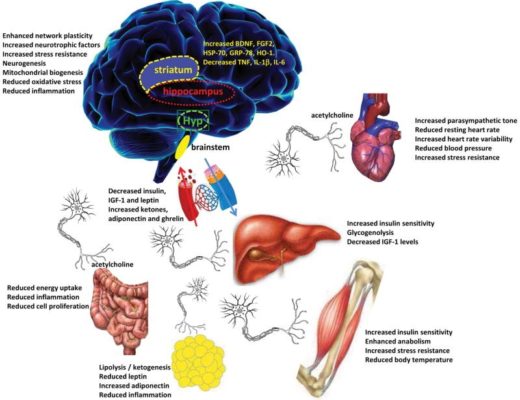
As we’ve discussed in prior posts, intermittent fasting contains NUMEROUS health benefits. Many patients begin lifestyle modifications, including decreasing processed carbohydrates and added sugar, increasing the consumption of plants, and the substitution of unhealthy fats for healthier options in an effort to improve weight loss, autoimmune disease, metabolic health, and overall longevity.
Intermittent fasting is a popular method known for improving insulin resistance, which is central to many disease states, including conditions associated with infertility, such as polycystic ovarian syndrome (for more information on
In general, fasting for prolonged periods during pregnancy is not recommended.
A prospective study of 130 patients in which Ramadan fasting occurred during pregnancy aimed to explore the short-term effects of fasting during pregnancy. At the time of the study, Ramadan took place during the summer months. Average fasting length was from 13-15 hours (sunrise to sunset). Women were analyzed according to the amount of fasting during the month and by trimester. Overall, no statistically significant differences in overall birth weight were found, though it should be noted that given the sample size, the study was likely underpowered to determine if a difference truly existed (1).
In a subset analysis, a birth weight difference of roughly 9.5 oz was present in women fasting during the first trimester, which did reach statistical significance, though the clinical significance of this finding still requires further research (1).
Similarly, a metanalysis of pregnancy outcomes was conducted on women in whom Ramadan fasting occurred. For reference, a meta-analysis attempts to answer a research question by combining the data of many smaller studies. Often, in order to draw conclusions regarding the clinical effect, larger sample sizes are needed. A meta-analysis aims to include the results of several studies in order to overcome sample size, particularly for rare outcomes.
Glazier, et al. examined 22 studies involving women opting to participate in Ramadan fasting. As in the prior study, birth weight was not significantly affected
While studies involving fasting are limited, we do not have data to state that regular, intentional fasting during pregnancy is safe, nor advised.
PROLONGED FASTING IN PREGNANCY CAN MAKE THINGS WORSE
Many pregnancy conditions can be exacerbated in the presence of prolonged fasting, including nausea and vomiting in pregnancy and the more severe form, hyperemesis gravidarium. While up to 80% of women experience nausea and vomiting during pregnancy, however, only 0.3-3% will experience hyperemesis gravidarium(3). The latter condition is characterized by severe nausea and vomiting combined with a weight loss of at least 5% of prepregnancy weight and electrolyte abnormalities (3). Prolonged periods between meals cannot only exacerbate normal nausea and vomiting of pregnancy, but it can also worse hyperemesis gravidarium, making treatment more difficult. In fact, part of the treatment strategy for both conditions includes small, frequent meals to stave of the cycle of nausea.
WEIGHT GAIN AND PREGNANCY
Pregnancy is a time of expected weight gain. Both suboptimal and excessive maternal weight gain
- Fat stores: 6-8 pounds
- Fetus/amniotic fluid: 9-10 pounds
- Increases in blood and extravascular volume: 5-7 pounds
- Breast enlargement: 1-3 pounds
- Placenta 1.5 pounds
Therefore, with healthy weight gain, the excess of maternal fat stores should not above ten pounds; however, many women fail to stay within the recommended guidelines for weight gain during pregnancy.
The Institute of Medicine recommends the following weight gain based on prepregnancy body mass index (BMI) in singleton pregnancies:
BMI < 18.5 kg/m2 (underweight): 28-40 pounds
18.5-24.9 kg/m2 (normal): 25-35 pounds
25-29 kg/m2 (overweight): 15-25 pounds
>30 kg/m2 (obese): 11-20 pounds
Excessive maternal weight gain increases the risk of gestational diabetes, need for medication to control gestational diabetes, preeclampsia, maternal ICU admission, and fetal macrosomia (6). As many as 60% of women gain above the recommended weight during pregnancy (6). Particularly with the obesity epidemic, the excess in processed foods, and limited amounts of vegetable intake; it is not difficult to see why excessive gestational weight gain is so common.

FOOD AS MEDICINE
Nutrition is the most vital component we have to modify health, even above fasting. This is why I stress the importance of finding a real foods diet that is sustainable, PRIOR to pregnancy, particularly because intermittent fasting is not recommended during pregnancy. It is particularly important as the foods a woman consumes during pregnancy while eventually serve as the building blocks for her growing child.
With regards to pregnancy and nutrition, the following are important to remember:
- In terms of “eating for two”, this is FALSE in terms of volume of food necessary to consume. For a woman carrying one baby, only an additional 250-300 calories a day are needed for the developing pregnancy.
- Nutrition wise, you ARE eating for two. Remember, we are what we eat. Aim for single ingredient foods, plenty of vegetables, make fruit your dessert, and aim for high quality, non-processed meats/foods.
- Work on improving your nutrition PRIOR to pregnancy. Figuring out what nutritional plan leaves you satisfied, feeling healthy, and is sustainable takes a WHILE! I’ve continued to redefine my nutrition over a two-year period, and continue to discover new ways to maximize my health. Part of planning a pregnancy involves making sure you optimize your health PRIOR to conception. Better health equals a lower risk of complications.
- Following a “gestational diabetic diet” is the nutritional therapy of choice for women with maternal or gestational diabetes; however, this is a way of eating that is beneficial for most women prior to, during, and after pregnancy. This is because it minimizes processed carbohydrates, processed meats while encouraging a healthy intake of protein, vegetables, and fruits as a treat.
SUMMARY
We do not know enough regarding the interactions of fasting on fetal health; therefore, pregnancy is not the time to experiment. Prioritize a real foods approach, prioritize responsible weight gain, and while you are eating for two, focus on NUTRITION as the building blocks of life.

REFERENCES
- Savitri AI, Yadegari N, Bakker J, van Ewijk RJ, Grobbee DE, Painter RC, et al. Ramadan fasting and newborn’s birth weight in pregnant Muslim women in The Netherlands. Br J Nutr. 2014;112(9):1503-9
- Glazier JD, Hayes
DJL , Hussain S, D’Souza SW, Whitcombe J, Heazell AEP, et al. The effect of Ramadan fasting during pregnancy on perinatal outcomes: a systematic review and meta-analysis. BMC pregnancy and childbirth. 2018;18(1):421. - London V, Grube S, Sherer DM, Abulafia O. Hyperemesis Gravidarum: A Review of Recent Literature. Pharmacology. 2017;100(3-4):161-71.
- Kominiarek MA, Gray EL, Vyhmeister H, Grobman W, Simon M. Association of Gestational Weight Gain with Prenatal Care Model. J Midwifery Womens Health. 2018;63(3):283-8.
- Gabbe S. Obstetrics: Normal and Problem Pregnancies, Sixth Edition: Saunders; 20112.
- Platner MH, Ackerman C, Howland RE, Xu X, Pettker CM, Illuzzi JL, et al. Gestational Weight Gain and Severe Maternal Morbidity at Delivery Hospitalization. Obstetrics and Gynecology. 2019;133(3):515-24.
DISCLAIMER: The advice on this page is not meant to replace or represent medical advice. This is nutritional advice, which is NOT the same as medical advice. Before any weight loss endeavor, the consultation of an experienced health care provider is a must. As a general rule, the following individuals should not participate in fasting:
- Diabetics-particularly those on insulin
- Lactating women
- Pregnant women
- Individuals with a history of eating disorders
- Children under the age of 18
This list is not
Interaction through this blog’s associated social media accounts, podcasts, and other venues associated with The Fasting Doctor does not constitute a patient-physician relationship. Likewise, it does not constitute medical advice. By continuing to access this blog or related resources, you acknowledge and agree that the content and contributors are not liable for your personal use of dietary and wellness advice found in our contents. You acknowledge our recommendation to consult your care provider before utilizing our nutritional information.
For more information, please contact me at info@thefastingdoctor.com!

No Comments